Some autistic women misdiagnosed with BPD spend years trying to understand themselves through an explanation that captures the distress without fully explaining the driver.
That is part of what makes this so painful.
On the surface, the pattern can look familiar: intense emotion, shutdown, relationship strain, identity confusion, overwhelm, social fallout. But what gets labeled as instability may sometimes be overloaded. What gets read as inconsistency may sometimes be masking. What gets interpreted as “too much” may actually be the visible end point of a nervous system under too much strain for too long.
That is where this gets missed.
Autistic women misdiagnosed with BPD are often being understood through the visible distress without enough attention to what is driving it.
60-Second Answer
Autism and BPD can overlap on the surface, especially in women whose autism was never clearly recognized.
That does not make them the same.
- BPD is generally understood through enduring patterns involving emotion regulation, relationships, and sense of self.
- Autism may involve masking, overload, shutdown, burnout, social processing differences, and a much higher cost of functioning than other people can see.
- Trauma can complicate the picture further.
- Some people are autistic and also meet criteria for BPD.
So the useful question is not just: What does this behavior look like?
It is: What is actually driving it?
And if you’re someone who replays conversations for hours, overthinks what you said, or gets stuck trying to decode what went wrong, start with the Overthinking Survival Kit.
When your brain will not let go, it helps to have something practical to interrupt the loop.
And if this kind of confusion turns into hours of replaying, second-guessing, or trying to solve yourself in one sitting, start with the Overthinking Survival Kit.
It’s a practical resource for overthinking, rumination, intrusive thoughts, and mental loops when your brain will not let something go.
TOC / Jump Links
- Why-autistic-women-misdiagnosed-with-BPD-get-misread
- Universal first move
- What gets mistaken for BPD
- Why masking can look like identity instability
- Why overload can look like emotional volatility
- Why relationship distress is not specific enough
- What BPD clinicians are actually looking for
- Trauma can make the picture harder to read
- What clinicians should be asking
- Try this now
- If You Already Reacted (Repair in 10 Seconds)
- Common mistakes
- FAQs
- What to do next
Why autistic women misdiagnosed with BPD get misread
Many autistic women do not match the version of autism people expect.
They may be verbal, thoughtful, empathic, funny, capable, socially motivated, and outwardly polished. They may make eye contact. They may seem emotionally aware. They may look like they are managing.
What often goes unseen is the effort.
A person can look fluent while working very hard behind the scenes. They may be tracking tone, rehearsing responses, monitoring facial expressions, suppressing discomfort, translating unclear social cues, scanning for mistakes, and trying not to fall one beat behind the conversation.
If the observer sees only the finished product, autism may not register.
What gets noticed instead is often the aftermath:
- shutdown
- tears after misunderstanding
- sudden withdrawal
- exhaustion
- shame
- social confusion
- burnout
- relationship strain
If someone is seeing only the aftermath, they may misunderstand the cause.
That misunderstanding matters. When the explanation is wrong, the person often ends up trying to solve the wrong problem. They may work even harder to become less emotional, less needy, less reactive, and less difficult. Meanwhile, the actual issues may be sensory strain, chronic masking, misattunement, trauma, or the sheer cost of moving through the world without enough room to recover.
Universal first move
Before turning familiar symptoms into a conclusion, slow the process down.
Start here:
- Separate the visible behavior from the likely driver.
- Ask what tends to happen right before the reaction.
- Look at masking, sensory load, trauma, and recovery cost.
- Treat distress as information, not proof.
A neat label is not the goal. A better-fitting explanation is.
That does not mean certainty is easy. It usually is not. But precision is still better than laziness.
What gets mistaken for BPD
The most important distinction is not who appears more emotional.
It is whether the visible reaction is being understood in context.
Two people can both cry easily, withdraw abruptly, have conflict-heavy relationships, and feel chronically misunderstood. That still does not tell you enough.
The real question is what gives rise to the pattern.
Is the person overloaded and nearing shutdown after sustained effort?
Are they disoriented by social ambiguity other people do not even notice?
Are they living with trauma that keeps the nervous system braced for danger?
Are they struggling with an enduring pattern better captured by BPD?
Are multiple things true at once?
That is the level of precision this topic requires.
Because resemblance is not an explanation.
What gets mistaken for BPD is often not one dramatic symptom. This is why autistic women misdiagnosed with BPD may spend years trying to fix the wrong problem. It is a cluster of things that can be easy to misread from the outside: emotional intensity, blurred identity, social fallout, abrupt exits, conflict sensitivity, and chronic shame. If those are treated as self-explanatory, the wrong story can take hold very quickly.
Why masking can look like identity instability
One reason this gets especially confusing in autistic women is masking.
Masking is not just “acting normal.” It can become a full organizing strategy. A person learns what makes other people more comfortable, then builds themselves around that.
They learn:
- which reactions are acceptable
- which needs get dismissed
- which preferences create friction
- which traits get penalized
- which parts of their natural style are easier to hide
Over time, this can blur a person’s sense of self.
Someone may say they do not know what they really want. They may not trust their own reactions. They may shape-shift socially. They may feel most coherent when alone and least coherent around other people.
From the outside, that can sound like instability of identity.
Sometimes it is interpreted that way immediately.
But there is an important difference between a self that feels unstable and a self that has been edited, corrected, and overridden for years.
That distinction changes the meaning of the problem.
In one case, the clinical question may center more on enduring instability in self and relationships. In the other, it may center more on adaptation, compensation, and the long-term cost of living too far from your actual limits.
Those are not interchangeable stories.
Why overload can look like emotional volatility
This is another place where interpretation breaks down.
When an autistic person reacts strongly, people often focus on the trigger closest to the reaction. That is understandable. But the final straw is often not the whole story.
What looks like a disproportionate reaction may have been building for hours or days:
- sensory strain
- social monitoring
- uncertainty
- noise
- interruptions
- unclear expectations
- pressure to perform normally
- not enough recovery time
Then one small thing happens. A tone change. A correction. A plan change. A demand added at the wrong moment.
From the outside, the reaction can look dramatic.
From the inside, the experience may be much closer to: I was already full.
That does not automatically make it autism. It does mean the buildup matters.
And that is the piece that often gets left out. A person who looks emotionally explosive may actually be hitting capacity after a long stretch of holding everything together. If no one asks about strain, buildup, sensory load, and recovery time, the interpretation can stay stuck at character.
Why relationship distress is not specific enough
A lot of confusion in this area comes from relationship distress.
Relationship pain is visible. It creates consequences. It is often what makes people start searching for an explanation.
But relationship distress is not specific enough to do that much work on its own.
An autistic woman may struggle in relationships because she:
- misses subtext
- processes language literally under stress
- becomes overloaded by conflict
- loses verbal access when flooded
- needs more recovery time than the relationship allows
- feels constantly behind in reading tone
From the outside, that can look contradictory or inconsistent.
But the visible pattern still does not explain itself.
It may reflect overload.
It may reflect trauma.
It may reflect attachment pain.
It may reflect BPD.
It may reflect some combination.
The point is not to flatten those into one thing because they rhyme from a distance.
This is especially important because relationship struggles are often where shame becomes most intense. People do not just wonder what happened. They start asking what is wrong with them. That is when overthinking can take over too, especially after a rupture, misunderstanding, or social mistake that will not stop replaying in their head.
What BPD clinicians are actually looking for
This part matters too.
A careful post on autism and BPD should not imply that BPD is just what people call distressed autistic women. That is not accurate.
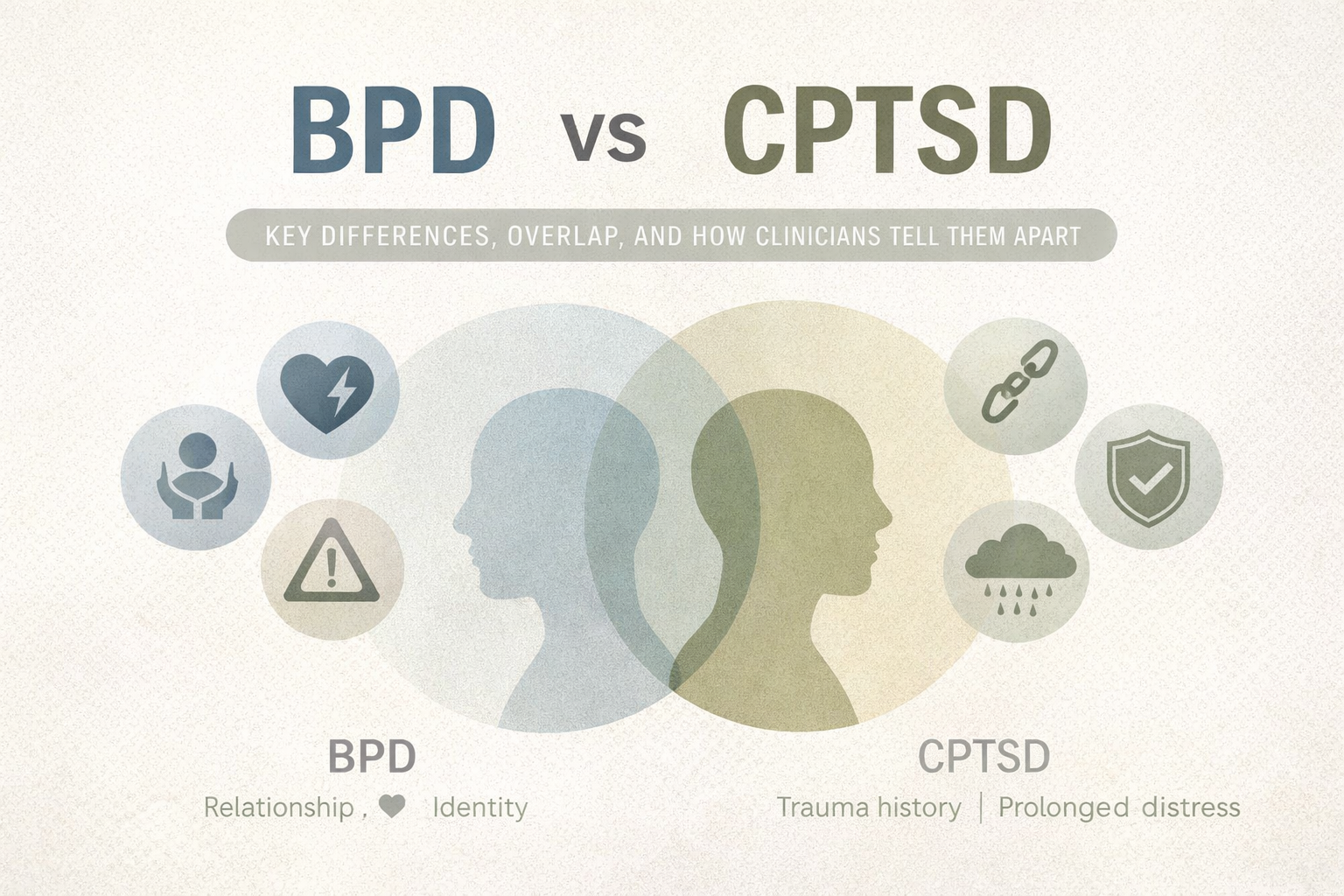
BPD is real. Some autistic women also meet criteria for BPD. And when BPD is central, clinicians are usually looking at a more specific pattern involving enduring difficulties with emotion regulation, relationships, and sense of self.
That may include:
- intense abandonment sensitivity
- rapidly shifting relationship dynamics
- identity disturbance
- severe emotion dysregulation
- chronic emptiness
- impulsive or self-destructive coping in some cases
That does not mean every person with BPD looks the same. It does mean the diagnosis is supposed to reflect more than visible intensity.
So the problem is not that clinicians ever diagnose BPD.
The problem is when intensity gets overread and context gets underread.
That is the distinction worth protecting.
Trauma can make the picture harder to read
Trauma complicates this conversation enormously.
For autistic women misdiagnosed with BPD, trauma can make the picture even harder to sort out clearly.
It can affect trust, self-concept, arousal, threat detection, sensitivity to uncertainty, and the body’s sense of safety. When trauma is present, people often become even more eager for a clean explanation.
The problem is that trauma rarely makes people easier to categorize.
Someone may look volatile when they are bracing for danger.
They may look avoidant when they are overloaded.
They may look inconsistent when they are moving between survival responses.
This is why tidy interpretations are often so attractive and so misleading. They create the feeling of clarity quickly. But speed is not the same as precision.
A person can be autistic and traumatized.
A person can have BPD and trauma.
A person can be autistic and also meet criteria for BPD.
A person can have been misunderstood through more than one lens for years.
That is why good assessment has to tolerate complexity without collapsing into vagueness.
What clinicians should be asking
Not just:
What does this look like?
But also:
- What reliably triggers it?
- What happens right before shutdown or escalation?
- What is the sensory load?
- How much masking is happening?
- What does recovery cost look like?
- What does developmental history suggest?
- What role does trauma play?
- Is the distress organized around overload, abandonment, unsafety, confusion, or some combination?
That is the level of precision this conversation needs.
Because two people can both look overwhelmed, relationally distressed, and emotionally intense.
One may be dealing primarily with autism.
One may be dealing primarily with BPD.
One may have trauma woven through everything.
One may have more than one diagnosis.
Surface similarity is not enough.
Try this now
If this article is making you want to re-examine every shutdown, every relationship, and every old diagnosis at once, pause before you obey that impulse.`
- Put both feet on the floor.
- Name five things you can see.
- Exhale longer than you inhale.
- Ask: Am I trying to understand the pattern, or am I already spiraling?
Sometimes the next useful step is not more analysis. It is regulation first.
If You Already Reacted (Repair in 10 Seconds)
If this topic sent you into a spiral, shutdown, conflict, or panic-searching loop, start here:
- Pause.
- Stop escalating the moment.
- Name what happened without shaming yourself.
- Try: “I’m overloaded, and I want to come back to this more clearly.”
- Give yourself ten minutes before the next conclusion, message, or late-night deep dive.
Repair usually starts with reducing intensity.
Common mistakes
Mistake 1: Treating surface resemblance like proof
Two patterns can look alike from the outside and still come from different drivers.
Mistake 2: Assuming polished presentation rules out autism
Many autistic women look socially fluent while paying a very high internal cost.
Mistake 3: Ignoring masking
If masking is not part of the assessment, the whole picture can get distorted.
Mistake 4: Mistaking overload for character
Overload is not a personality flaw.
Mistake 5: Using relationship distress as a diagnosis
Relationship pain matters, but it is not specific enough on its own.
Mistake 6: Forgetting trauma
Trauma can complicate regulation, self-concept, trust, and reactivity in ways that blur the picture.
If this topic sends you into hours of replaying, decoding, or mentally arguing with yourself, start with the Overthinking Survival Kit.
It’s a practical resource for overthinking, rumination, intrusive thoughts, and mental loops when your brain will not let something go.
FAQs
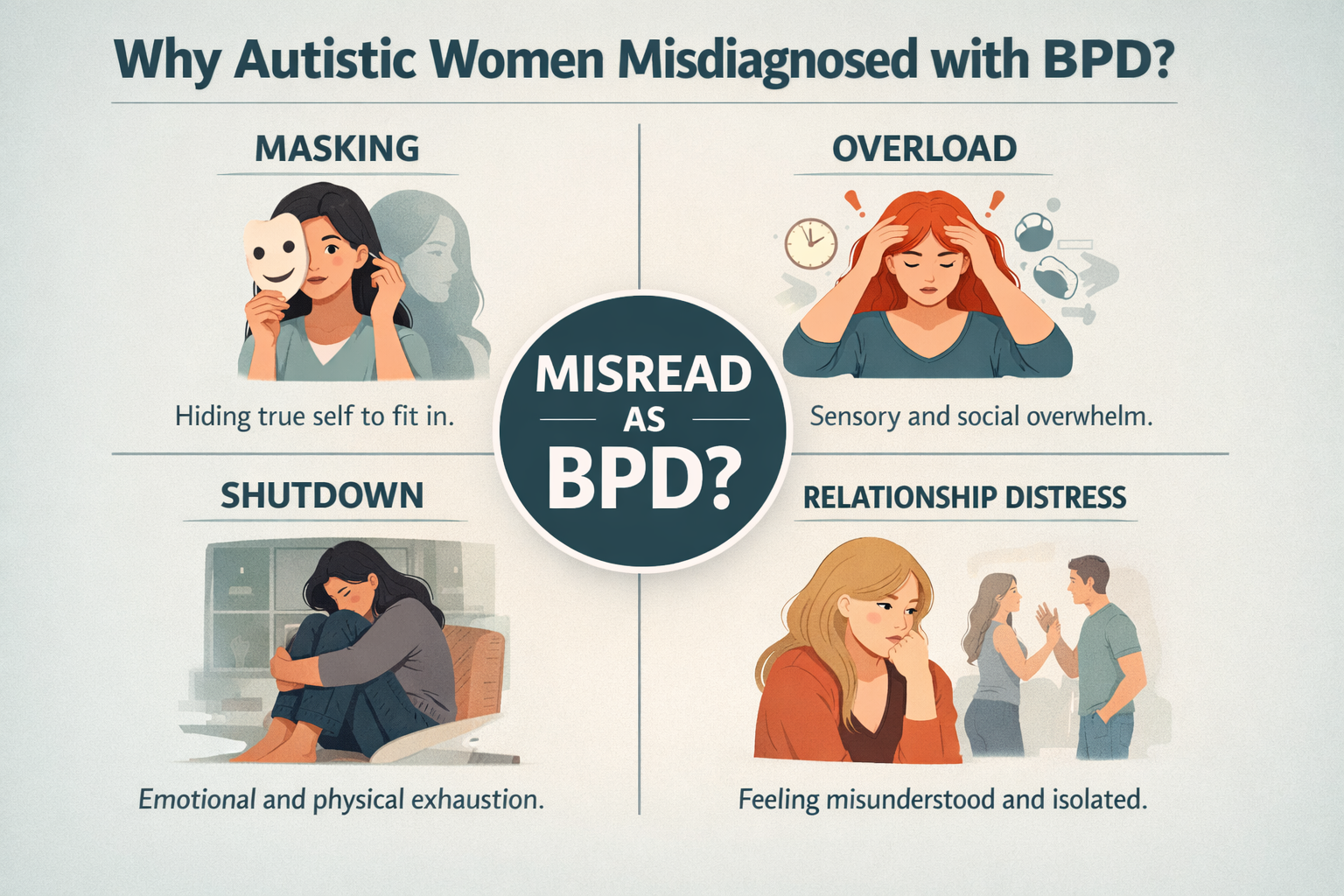
Why are autistic women sometimes misdiagnosed with BPD?
Because the outward pattern can overlap while the underlying driver may be very different. Masking, overload, burnout, social strain, and hidden effort are often missed.
Can autistic women also have BPD?
Yes. Some people are autistic and also meet criteria for BPD. The point is not to swap labels casually, but to understand the pattern more accurately.
What gets confused between autism and BPD in women?
Emotional intensity, relationship distress, shutdown, self-doubt, blurred identity, and strong reactions under pressure can all be interpreted too quickly without enough attention to masking, sensory load, trauma, and recovery cost.
Is relationship distress enough to tell the difference?
No. Relationship distress is real, but it is not specific enough on its own to explain the underlying issue.
Is this article meant to diagnose autism or BPD?
No. It is educational content meant to help readers think more carefully about patterns that are often oversimplified.
Can masking really affect one’s sense of self?
Yes. Over time, chronic masking can blur preferences, limits, and self-trust in ways that get mistaken for something else.
Can trauma make this harder to sort out?
Yes. Trauma can intensify threat detection, shame, reactivity, and relational distress in ways that complicate the whole picture.
What to do next
The issue is not which label sounds kinder, smarter, or more accurate from a distance.
The issue is whether the explanation actually fits the lived pattern.
A person can spend years trying to fix “emotional instability” when the more relevant problem is overload. They can spend years analyzing relationship pain without realizing how much social processing strain is involved. They can spend years being read through a framework that catches the intensity while missing the mechanism.
That is the cost of imprecision.
Autistic women misdiagnosed with BPD often need a more careful explanation of the pattern, not just a faster label.
And if you’re someone who gets stuck replaying conversations, searching for the perfect explanation, or mentally looping long after the interaction ended, start with the Overthinking Survival Kit.
It’s there for overthinking, rumination, intrusive thoughts, and the kind of mental loops that keep your brain from letting go.
For immediate crisis support in the US, contact the 988 Suicide & Crisis Lifeline: https://988lifeline.org/
This article is for educational purposes only. It is not a substitute for diagnosis, therapy, or mental health treatment.